
Download
ORIGINAL ARTICLE
Effect of adding fenugreek and Nigella sativa to white rice on postprandial glycemic and appetite responses in healthy individuals
Imran Khan1,2*, Muhammad Shahid Afridi2, Jamil Ahmad2, Stuart K. Johnson3, Mohammed H. Al-Rizeiqi1, Ali Madi Almajwal4
1Department of Food Science and Nutrition, College of Agricultural and Marine Sciences, Sultan Qaboos University, Al-Khoud, Muscat, Oman;
2Department of Human Nutrition, The University of Agriculture, Peshawar, Khyber Pakhtunkhwa, Pakistan;
3School of Public Health, Curtin Health Innovation Research Institute, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia;
4Department of Community Health Sciences, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia
Abstract
White rice is a high glycemic index food, and therefore different approaches are adopted to reduce its glycemic effect. The present study investigated the effect of adding fenugreek and Nigella sativa seed powder to white rice on glycemia, appetite, palatability, and gastrointestinal clinical manifestations in healthy subjects. In a randomized crossover design, 16 healthy subjects consumed white rice alone (control group), white rice with 2-g fenugreek seed powder or white rice with 4-g nigella seed powder on different occasions. Each test meal provided 50 g of available carbohydrates. Blood glucose, subjective appetite, and gastrointestinal manifestations were measured at fasting and postprandially for 2 h. Palatability of the test meals was also measured using a 9-point hedonic scale. The nigella meal resulted in significantly lower blood glucose concentration (31.25 mg/dL) at 30 min (p = 0.022), compared to the control meal (43.88 mg/dL) whereas fenugreek meal showed no significant effect. Moreover, the nigella meal significantly increased satiety ratings at 30 and 90 min (p = 0.035 and 0.018, respectively). The results demonstrated that the addition of nigella powder to white rice reduced its glycemic response and increased satiety, compared to the control meal. All test meals were judged as acceptable by the subjects and their consumption didn’t cause any gastrointestinal discomfort. Results of the current study demonstrated promising implications for reducing glycemic response of white rice, a commonly consumed high-glycemic index food.
Key words: appetite, fenugreek, glycemia, Nigella sativa, rice
*Corresponding Author: Imran Khan, Department of Food Science and Nutrition, College of Agricultural and Marine Sciences, Sultan Qaboos University, Al-Khoud 123, Muscat, Oman. Emails: [email protected]; [email protected]
Received: 19 March 2024; Accepted: 21 May 2024; Published: 20 August 2024
© 2024 Codon Publications
This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY-NC-SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/)
Introduction
Rice is a staple food consumed daily by more than half of global population. In many Asian countries, it is a major single source of carbohydrates and energy; however, its intake has been associated with increased risk of type 2 diabetes (Hu et al., 2012). This could be explained by high glycemic response of rice, because higher levels of postprandial glycemic response increase the risk of developing chronic diseases, particularly type 2 diabetes (Blaak et al., 2012; Zhang et al., 2016). Therefore, different ingredients are added to rice to reduce its glycemic response (Hlebowicz et al., 2007; Sun et al., 2014; Zenel and Stewart, 2015; Zhang et al., 2016).
Medicinal plants are important sources of bioactive compounds and their addition to high glycemic foods reduces the glycemic response of such foods. Fenugreek, as seeds and green leaves, is a medicinal plant used as a spice in human food (Thomas et al., 2011). Its high fiber content and presence of other bioactive compounds, such as alkaloids, saponins, steroidal sapinogens, and polyphenols, make fenugreek a health-promoting herb (Murlidhar and Goswami, 2012; Wani and Kumar, 2018). Fenugreek fiber increases satiety and reduces energy intake at lunch, suggesting that it may have short-term beneficial effects on lowering energy intake in obese subjects (Mathern et al., 2009). Previous studies have also found that 25–50-g fenugreek seeds in daily diet of diabetic subjects exert beneficial effect on their glycemic response (Das et al., 2012).
Nigella sativa is another medicinal plant used traditionally for the treatment of diabetes. The antidiabetic effect of Nigella sativa is attributed to its insulinotropic action (Fararh et al., 2002; Rchid et al., 2004) and antioxidant properties which decrease oxidative stress and thus help preserve pancreatic β-cell integrity (Altan et al., 2007; Kanter et al., 2003). In different animal studies, Nigella sativa has been shown to decrease blood glucose in diabetic induced rats (Alimohammadi et al., 2013; Asaduzzaman et al., 2015). In human studies, different doses of Nigella sativa (1–3 g per day) have been shown to decrease blood glucose concentration in type 2 diabetic subjects (Bamosa et al., 2010).
However, no study has been conducted on the acute effects of adding fenugreek and Nigella sativa to white rice and its glycemic and appetite responses. Therefore, the objective of the present study was to determine the effect of adding fenugreek and nigella seed powder to white rice on postprandial glycemic and appetite responses in healthy subjects and assess palatability of meals and gastrointestinal clinical manifestations of subjects. It was hypothesized that the addition of these spices to white rice would result in lowered postprandial glycemia and increased satiety, compared to white rice without any addition.
Materials and Methods
Study subjects
This study was conducted at the Laboratory of Human Nutrition, the University of Agriculture, Peshawar (Pakistan) and included healthy subjects irrespective of gender, aged 18–60 years. The subjects were recruited through posted flyers and direct personal meetings. The subjects were screened using a health questionnaire after receiving written informed consent. Exclusion criteria included a history of cardiovascular disease (CVD), diabetes, asthma, food allergies, major gastrointestinal problems, hypertension, currently on dieting or skipping breakfast regularly, medication known to affect glucose metabolism, and smoking. In addition, subjects having fasting blood glucose concentration >101 mg/dL were also excluded from the study. The sample size for the present study was calculated using the NCSS 2004/PASS 2002 statistical software for power and sample size estimation (Hintze, 2001).
A total of 16 subjects were required to detect a 20% difference in the blood glucose concentration with a power of 80% and α ≤ 0.05. The study was conducted according to the guidelines of Declaration of Helsinki and approved by the Ethics Committee and Human Studies Review Board (FNS-ECHSRB/2015-0087) of the University of Agriculture Peshawar.
Study design and protocol
The study was designed as a randomized, controlled, cross-over trail in accordance to the protocol adopted by Ahmad et al. (2018). Each subject attended three testing sessions, each 1–2-week apart. On each study visit, subjects ate one of the three test meals. Subjects were requested to avoid hard physical activity before each study visit. To minimize any differences in the second meal effect, subjects were instructed to eat and drink the same foods the evening prior to each visit to record this in a dairy. Subjects were directed to consume their dinner before 9:00 pm on the evening prior to each test day; after testing session they were requested to abstain from food (i.e., fasting). Subjects attended each study visit at 08:30 am, following 10–12-h fasting.
At first visit, baseline measurements, such as weight, height, and waist circumference, were recorded upon arrival at the laboratory. Fasting blood glucose was measured by finger prick after taking 5-min rest. The subjects then assessed their appetite sensation using visual analogue scales (VAS). Thereafter, test meal, comprising 50 g of available carbohydrates, was consumed with 200-mL water within 10 min. During consumption, subjects were required to rate the palatability of test meal using a 9-point hedonic scale. Blood glucose was measured at 15, 30, 45, 60, 90, 120 min after consumption of test meal. Immediately after taking blood samples at the above-mentioned time intervals, subjects were required to fill out VAS. Subjects also assessed any gastrointestinal discomfort felt by them at fasting and at 30, 60, 90, and 120 min of consumption of test meal.
Test meals
Dry seeds of fenugreek and Nigella sativa were purchased from the local market and crunched into powder using a commercial grinder. The control meal was prepared from white rice only (Kainat Super Kernel Basmati rice; Mehran Foods International, Pakistan). Fenugreek meal comprised cooked rice with addition of 2-g fenugreek seed powder whereas nigella meal comprised cooked white rice with 4-g nigella seed powder. Fenugreek and nigella seed powder used in the present study was chosen from the results of a pilot consumer sensory evaluation study (data not shown). The amount of each test meal served was calculated on the basis of providing 50 g available carbohydrates. Each portion of rice (raw weight: 64 g) was cooked individually for 20 min using 130 mL of water. Salt (1 g) and oil (5 g) were added for taste during cooking. Fenugreek seed and nigella seed powder were added to the freshly cooked warm rice before serving to the subjects. The nutrient composition of test meals is given in Table 1.
Table 1. Nutrient composition of test meals.
| Composition | C | F | N |
|---|---|---|---|
| Total cooked weight (g) | 190 | 192 | 194 |
| Energy (g) | 226.94 | 228.79 | 241.74 |
| Av. CHO (g) | 50 | 50 | 50 |
| Protein (g) | 4.29 | 4.55 | 5.11 |
| Fats (g) | 1.09 | 1.18 | 2.37 |
| Dietary fiber (g) | 0.26 | 0.52 | 0.67 |
Av. CHO: available carbohydrates; C: control meal; F: fenugreek meal; N: nigella meal.
Baseline measurements
Subjects’ weight, height, and waist circumference were measured using standard methods. Weight was measured using digital scale. The subjects were asked to remove heavy clothing, shoes and other unnecessary things. The height was measured using a stadiometer. Weight and height were used to calculate body mass index (BMI). Circumference of waist was measured midway between the lowest rib margin and iliac crest and recorded to the nearest 0.1 cm.
Blood glucose analysis
The capillary blood samples were obtained by finger-prick with the help of single-use lancet device. Before collecting the blood sample, the subjects were encouraged to warm their hands to increase blood flow. Accu-check performa blood glucose analyzer (Roche Diabetes Care, Indianapolis, IN, USA) was used to measure blood glucose level.
Subjects’ appetite measurements
Subjects’ appetite was evaluated for satiety, fullness, hunger, and prospective food intake with 100-mm VAS (Flint et al., 2000). The following questions were related to these scales: How hungry do you feel? (“not hungry at all” = 0 mm to “as hungry as I have ever been” = 100 mm); how satisfied do you feel? (“completely empty” = 0 mm to “cannot eat another bite” = 100 mm); how full do you feel? (“not full at all” = 0 mm to “totally full” = 100 mm); and how much do you think you could eat? (“nothing at all” = 0 mm to “a large amount” = 100 mm). The subjects were asked to place a vertical mark on each scale, somewhere between 0 mm and 100 mm, extremes, and were not permitted to refer to their previous ratings when marking the scale. These scores were converted to continuous variables by measuring distance in millimeter from the far-left anchor of the scale. A validated composite appetite score, as a global measure of satiety, was calculated using the following equation (Gonzalez-Anton et al., 2015):
Composite appetite score = (Satiety + fullness + [100 – prospective food consumption] + [100 – hunger])/4.
The single composite appetite score was used to ease data analyis and presentation.
Palatability assessment
Palatability of test meals was assessed in terms of appearance, flavor, texture, and overall acceptability using 9-point hedonic scale, with extremely dislike on one end and extremely like on the other (Meilgaard et al., 2007). The subjects were asked to mark a position on the scale, best matching their perception.
Gastrointestinal manifestations
Any gastrointestinal discomfort was evaluated using a validated questionnaire at 0 min (immediately prior to consumption of test meal) and at 30, 60, 90, and 120 min after consumption of test meal (Bovenschen et al., 2006). Evaluated manifestations were the occurrence (none, mild, moderate, quite a lot, severe, very severe, and unbearable) of abdominal pain, heart burn, vomiting, and nausea.
Calculation and statistical analysis
Incremental blood glucose and composite appetite score values for each test meal were calculated by subtracting each subject’s fasting values from the value of each postprandial time point. The incremental values were then used to construct glucose and composite appetite score response curves. Incremental areas under the curves (iAUCs) for blood glucose and composite appetite score were calculated using the trapezoidal method, ignoring area below zero (incremental baseline value).
Statistical analysis was performed using the SPSS statistical software version 16 (SPSS Inc. Chicago, IL, USA). Two-way repeated measures ANOVA was used to examine the effect of treatment, time, and time-by-treatment interaction on blood glucose, composite appetite score, and gastrointestinal manifestations. A statistically significant interaction was then followed by one-way repeated measures ANOVA, with Bonferroni adjustment for multiple comparisons to explain mean differences between treatments at each time point. The effect on blood glucose and composite appetite score iAUCs were determined by one-way repeated measures ANOVA, followed by post hoc analysis with Benferroni adjustment for multiple comparisons. One-way repeated measures ANOVA with post hoc Benferroni test was used to determine any significant effect in the palatability parameters of test meals; p < 0.05 was considered as statistically significant.
Results
Subject characteristics
All subjects completed all three sessions of the study. Their baseline characteristics are shown in Table 2.
Table 2. Characteristics of study subjects (n = 16).*
| Variable | Values |
|---|---|
| M/F | 8/8 |
| Age (year) | 22.6 ± 0.89 |
| Weight (kg) | 66.1 ± 12.5 |
| Height (cm) | 164.8 ± 10.6 |
| Waist circumference (cm) | 82.2 ± 11.8 |
| BMI (kg/m2) | 23.9 ± 3.2 |
| Fasting plasma glucose (mg/dL) | 91.01 ± 1.41 |
*Mean ± SD values. BMI: body mass index.
Blood glucose response
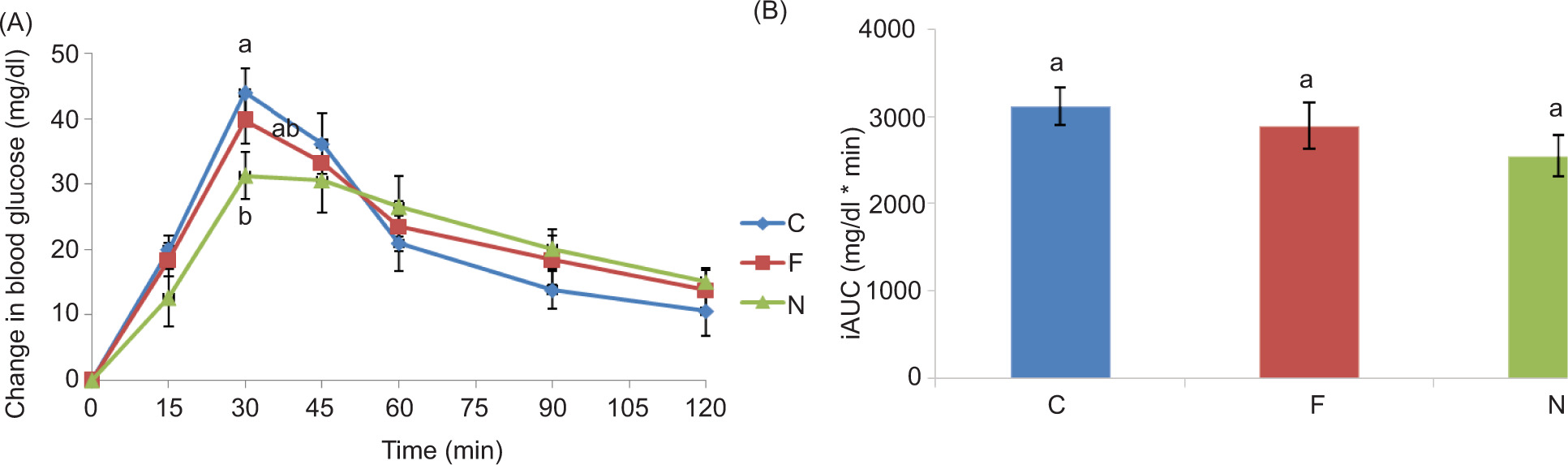
The postprandial blood glucose responses after consumption of test meals with the corresponding iAUCs are shown in Figure 1. There was significant effect of time (p < 0.001), treatment (p = 0.037) and time-by-treatment interaction (p = 0.003) on blood glucose concentrations. Post hoc pair-wise comparison showed that the nigella meal resulted in significantly lower blood glucose concentration compared to control meal (p = 0.031). In order to investigate response to treatments in detail over time, the effect of treatment was determined at each time point by one-way repeated measure ANOVA. The nigella meal resulted in significantly lower blood glucose concentration at a time point of 30 min, compared to control meal (p = 0.022). In addition, there was a tendency for lowered blood glucose iAUC after the consumption of nigella meal, compared to control meal (p = 0.077).
Figure 1. Mean (±SEM) changes from baseline in (A) plasma glucose and (B) iAUC in healthy subjects (n = 16) after consumption of test meals (C: control meal; F: fenugreek meal; N: nigella meal). Values with different superscript letters are significantly different at each time point: two-way repeated measure ANOVA, followed by one-way repeated measure ANOVA, and Bonferroni adjustment (p < 0.05). Vertical bars are not significantly different, p < 0.05 (one-way repeated ANOVA with post hoc Bonferroni).
Subjective appetite measures
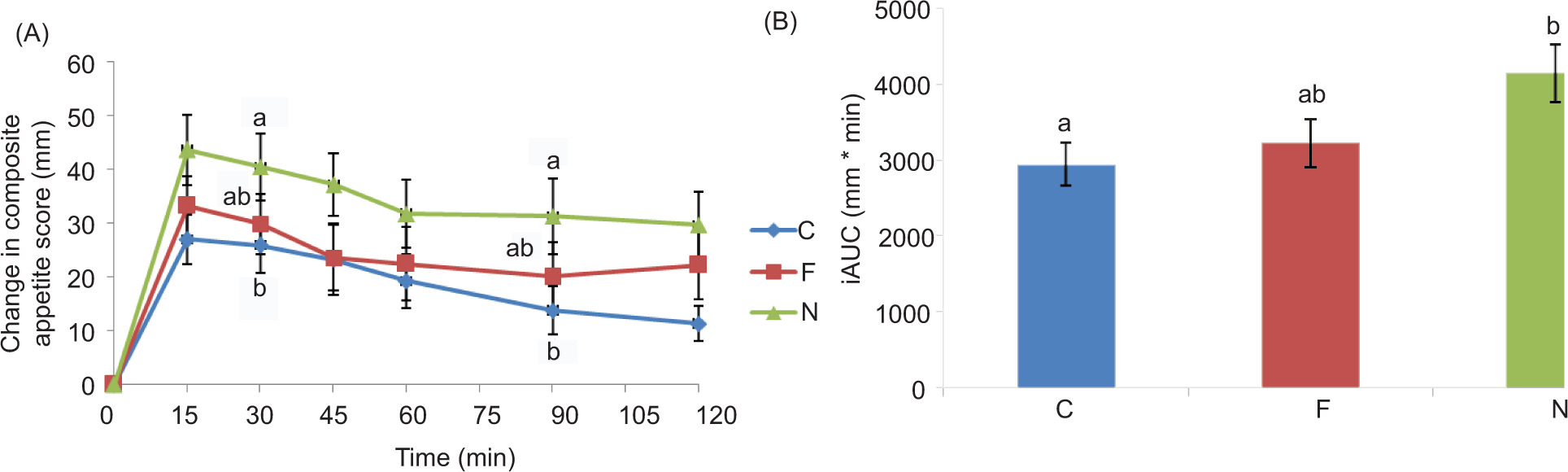
The postprandial appetite response measured in terms of composite appetite score after the consumption of the test meals with the corresponding iAUCs are shown in Figure 2. A significant effect of time (p < 0.001) and treatment (p = 0.014) was observed but no effect of time-by-treatment interaction (p = 0.098) on composite appetite score was discovered. The nigella meal resulted in significantly increased composite appetite score responses at 30 and 90 min (p = 0.035 and 0.018, respectively), compared to control meal. In addition, a significant increase in composite appetite score iAUC was observed after the consumption of nigella meal, compared to control meal (p = 0.026).
Figure 2. Mean (±SEM) changes from baseline in (A) composite appetite score with (B) corresponding iAUC in healthy subjects (n = 16) after the consumption of test meals (C: control meal; F: fenugreek meal; N: nigella meal). Values with different superscript letters are significantly different at each time point: two-way repeated measure ANOVA, followed by one-way repeated measure ANOVA, Bonferroni adjustment (p < 0.05). Vertical bars with different letters are significantly different, p < 0.05 (one-way repeated ANOVA, Bonferroni adjustment).
Palatability of test meals
Palatability characteristics of test meals are shown in Table 3. No significant differences between test meals were observed in terms of appearance, texture, flavor, and overall acceptance (p > 0.05).
Table 3. Palatability parameters of test meals.*
| Test meal | Appearance | Texture | Flavor | Overall acceptance |
|---|---|---|---|---|
| C | 7.31 ± 0.52 | 7.94 ± 0.59 | 7.19 ± 0.50 | 7.38 ± 0.46 |
| F | 6.25 ± 0.45 | 6.19 ± 0.49 | 6.06 ± 0.65 | 5.94 ± 0.54 |
| N | 6.06 ± 0.21 | 6.18 ± 0.28 | 6.31 ± 0.31 | 6.56 ± 0.35 |
*Mean ± SEM values (n = 16). Values are not significantly different between test meals for any of the palatability parameters (p < 0.05), one-way repeated (ANOVA), and Bonferroni adjustment. Values are scored on 9-point hedonic scale, where 9 = like extremely, 8 = like very much, 7 = like moderately, 6 = like slightly, 5 = neither like nor dislike, 4 = dislike slightly, 3 = dislike moderately, 2 = dislike very much, and 1 = dislike extremely. C: control meal; F: fenugreek meal; N: nigella meal.
Gastrointestinal manifestations
No significant difference between test meals was observed in terms of gastrointestinal manifestations, including abdominal pain, heartburn, vomiting, and nausea (p > 0.05) (data not shown).
Discussion
The present study reported the effect of fenugreek and nigella seed powder added to cooked white rice on postprandial glycemia, subjective appetite, palatability, and gastrointestinal manifestations in healthy subjects. It was hypothesized that the addition of fenugreek and Nigella sativa in powder form to cooked rice would decrease postprandial glycemia and increase satiety with no effect on palatability and gastrointestinal manifestations. However, the hypothesis was true in the case of nigella meal only. The results showed that nigella meal, but not fenugreek meal, significantly reduced postprandial glycemia and increased satiety compared to control meal.
The effects of Nigella sativa on blood glucose was previously reported in diabetic subjects (Mahdavi et al., 2016). However, to the best of our knowledge, this is the first reported study that demonstrated the effect of Nigella sativa added to rice on blood glucose in healthy subjects. Although the exact mechanism responsible for decrease in blood glucose concentration after the consumption of nigella meal is not clear, many possible mechanisms are responsible for this lowered blood glucose. It has been shown that Nigella sativa could decrease intestinal glucose absorption by inhibiting sodium-dependent glucose transport in vitro (Meddah et al., 2009). Moreover, it was proposed that the suppressive effects of Nigella sativa on glucose absorption could be due to its polyphenols (Heshmati et al., 2015). Reduced blood glucose observed after consumption of nigella meal could be partly due to the inhibition of α-amylase and α-glycosidase enzyme activities, as it was demonstrated in vitro that Nigella sativa had this inhibitory potential (Amutha and Godavari, 2016; Sobhi et al., 2016).
Reduced appetite observed after consuming nigella meal in the present study was consistent with a recent randomized, double-blind, placebo-controlled study, in which Nigella sativa oil was shown to reduce appetite and energy intake throughout the study in diabetic subjects (Heshmati et al., 2015). In another randomized, double-blind controlled study, the intervention group (consuming Nigella sativa in the form of capsules) had reduced appetite and a significant reduced food intake, compared to the control group (Qidwai et al., 2009). Similarly, in an animal study, the petroleum ether extract of Nigella sativa reduced appetite and caused a 25% reduction in food intake in normal mice (Le et al., 2004). Moreover, the consumption of fortified Nigella sativa bread with high protein diets decreased feed intake and body weight in diabetic mice (Mahmoud, 2013). Active components and physiological mechanism of Nigella sativa responsible for reducing appetite are not reported yet, and therefore future studies must identify its active components and their mechanisms responsible for reducing appetite.
Contrary to the hypothesis of the present study, no significant effect of fenugreek meal was observed on postprandial glycemia and appetite. In a recent study conducted in overweight and obese subjects, 2 g of fenugreek powder added to white bread and jam (providing 50 g available carbohydrates) also showed no effect on postprandial glycemia. However, when the dose was increased to 5.5 g, a significant reduction in postprandial glycemia and appetite was observed, but this dose caused bitter taste (Robert et al., 2014). In another study, a dose of 5 g but not 2.5 g of fenugreek seeds significantly decreased postprandial blood glucose in diabetic subjects, compared to control subjects (Bawadi et al., 2009). According to a meta-analysis, only medium to high doses (range: 5–100 g) of fenugreek seed powder were responsible for significant reduction in blood glucose (Neelakantan et al., 2014). Based on the results of the above-mentioned studies, a low dose (2 g) of fenugreek used in the present study could be one of the possible reasons for not reduced blood glucose concentration. Future studies are needed to study the effect of high doses of fenugreek on postprandial glycemia and appetite in rice while maintaining palatability of meals.
The present study had some limitations: parameters, such as gastric emptying rate, objective food intake from an ad libitum lunch, insulin levels, and appetite regulatory hormones, were not measured and as such should be investigated in future studies.
Conclusion
The addition of Nigella sativa powder, but not fenugreek, to white rice reduced its glycemic effect and increased satiety, compared to control rice. All test meals were equally palatable and no gastrointestinal discomfort was reported with consumption of any meal. The results of the present research have practical implications for reducing glycemic response and enhancing the satiety effect of white rice, particularly in the areas where it is consumed as a staple food. Moreover, the results of this study could also be used as a reference in future studies regarding the beneficial effects of adding fenugreek and Nigella sativa to different foods on biomarkers of diabetes, obesity, and CVD in healthy, diabetic, or obese subjects.
Data Availability Statement
The data presented in this study are available upon reasonable request from the corresponding author. The data are not publicly available due to privacy.
Conflict of Interest
The authors declared that there was no conflict of interest.
Author Contributions
Muhammad Shahid Afridi, Jamil Ahmad, and Imran Khan designed the study. Muhammad Shahid Afridi and Jamil Ahmad conducted the study and analyzed the data. Jamil Ahmad and Muhammad Shahid Afridi drafted the manuscript. Imran Khan, Ali Madi Almajwal, and Stuart K. Johnson critically revised the manuscript. All authors had read and approved the final version of the manuscript.
Acknowledgments
The authors extend their appreciation to the Researchers Supporting Project No. RSP2024R502, King Saud University, Riyadh, Saudi Arabia.
REFERENCES
Ahmad J., Khan I., Johnson S.K., Alam I., and Din Z.U. 2018. Effect of incorporating stevia and moringa in cookies on postprandial glycemia, appetite, palatability, and gastrointestinal well-being. J Am Coll Nutr. 37(2): 133–139. 10.1080/07315724.2017.1372821
Alimohammadi S., Hobbenaghi R., Javanbakht J., Kheradmand D., Mortezaee R., Tavakoli M., Khadivar F., and Akbari H. 2013. Protective and antidiabetic effects of extract from Nigella sativa on blood glucose concentrations against streptozotocin (STZ)-induced diabetic in rats: an experimental study with histopathological evaluation. Diagn Pathol. 8(1): 1–7. 10.1186/1746-1596-8-137
Altan M.F., Kanter M., Donmez S., Kartal M.E., and Buyukbas S. 2007. Combination therapy of Nigella sativa and human parathyroid hormone on bone mass, biomechanical behavior and structure in streptozotocin-induced diabetic rats. Acta Histochem. 109(4): 304–314. 10.1016/j.acthis.2007.02.006
Amutha K and Godavari K. 2015. Antidiabetic and phytochemical screening of Nigella sativa. J Chem Pharm Res. 7(8): 432–436.
Asaduzzaman M., Nahar L., Rahman M.S., Hasan M., Khatun A., Tamanna Z., Huda N., Rabbi F.M., Ray M.N., Nur Islam M., Mobassirul I.M. 2015. Hypoglycemic and hypolipidemic potential of Nigella sativa L. seed extract in streptozotocin (STZ)-induced diabetic rats. J Plant Biochem Physiol. 3: 158.
Bamosa A.O., Kaatabi H., Lebdaa F.M., Elq A.M., and Al-Sultanb A. 2010. Effect of Nigella sativa seeds on the glycemic control of patients with type 2 diabetes mellitus. Indian J Physiol Pharmacol. 54(4): 344–354.
Bawadi H.A., Maghaydah S.N., Tayyem R.F., and Tayyem R.F. 2009. The postprandial hypoglycemic activity of fenugreek seed and seeds’ extract in type 2 diabetics: a pilot study. Pharmacogn Mag. 5(18): 134–138.
Blaak E.E., Antoine J.M., Benton D., Björck I., Bozzetto L., Brouns F., Diamant M., Dye L., Hulshof T., Holst J.J., and Lamport D.J. 2012. Impact of postprandial glycaemia on health and prevention of disease. Obes Rev. 13(10): 923–984. 10.1111/j.1467-789X.2012.01011.x
Bovenschen H.J., Janssen M.J., Van Oijen M.G., Laheij R.J., Van Rossum L.G., and Jansen J.B. 2006. Evaluation of a gastrointestinal symptoms questionnaire. Dig Dis Sci. 51(9): 1509–1515. 10.1007/s10620-006-9120-6
Das L., Bhaumik E., Raychaudhuri U., and Chakraborty R. 2012. Role of nutraceuticals in human health. J Food Sci Technol. 49(2): 173–183. 10.1007/s13197-011-0269-4
Fararh K.M., Atoji Y., Shimizu Y., and Takewaki T. 2002. Isulinotropic properties of Nigella sativa oil in streptozotocin plus nicotinamide diabetic hamster. Res Vet Sci. 73(3): 279–282. 10.1016/S0034-5288(02)00108-X
Flint A., Raben A., Blundell J.E., and Astrup A. 2000. Reproducibility, power and validity of visual analogue scales in assessment of appetite sensations in single test meal studies. Int J Obes. 24(1): 38–48. 10.1038/sj.ijo.0801083
Gonzalez-Anton C., Lopez-Millan B., Rico M.C., Sanchez-Rodriguez E., Ruiz-Lopez M.D., Gil A., and Mesa M.D. 2015. An enriched, cereal-based bread affects appetite ratings and glycemic, insulinemic, and gastrointestinal hormone responses in healthy adults in a randomized, controlled trial. J Nutr. 145(2): 231–238. 10.3945/jn.114.200386
Heshmati J., Namazi N., Memarzadeh M.R., Taghizadeh M., Kolahdooz F. 2015. Nigella sativa oil affects glucose metabolism and lipid concentrations in patients with type 2 diabetes: a randomized, double-blind, placebo-controlled trial. Food Res Int. 70: 87–93. 10.1016/j.foodres.2015.01.030
Hintze J. 2001. NCSS and PASS number crucher statistical systems. Available at: http://www.NCSS.com.
Hlebowicz J., Darwiche G., Björgell O., Almér L.O. 2007. Effect of cinnamon on postprandial blood glucose, gastric emptying, and satiety in healthy subjects. Am J Clin Nutr. 85(6): 1552–1556. 10.1093/ajcn/85.6.1552
Hu E.A., Pan A., Malik V., and Sun Q. 2012. White rice consumption and risk of type 2 diabetes: meta-analysis and systematic review. BMJ. 344: 1454. 10.1136/bmj.e1454
Kanter M., Meral I., Yener Z., Ozbek H., and Demir H. 2003. Partial regeneration/proliferation of the β-cells in the Islets of Langerhans by Nigella sativa L. in streptozotocin-induced diabetic rats. Tohoku J Exp Med. 201(4): 213–219. 10.1620/tjem.201.213
Le P.M., Benhaddou-Andaloussi A., Elimadi A., Settaf A., Cherrah Y., and Haddad P.S. 2004. The petroleum ether extract of Nigella sativa exerts lipid-lowering and insulin-sensitizing actions in the rat. J Ethnopharmacol. 94(2–3): 251–259. 10.1016/j.jep.2004.04.030
Mahdavi R., Alizadeh M., Namazi N., and Farajnia S. 2016. Changes of body composition and circulating adipokines in response to Nigella sativa oil with a calorie restricted diet in obese women. J Herb Med. 6(2): 67–72. 10.1016/j.hermed.2016.03.003
Mahmoud M.Y. 2013. Effect of high protein diet containing fortified bread with fenugreek and Nigella sativa seeds on rats suffering from diabetes. Pak J Nutr. 12(8): 736–747. 10.3923/pjn.2013.736.747
Mathern J.R., Raatz S.K., Thomas W., and Slavin J.L. 2009. Effect of fenugreek fiber on satiety, blood glucose and insulin response and energy intake in obese subjects. Phytother Res. 23(11): 1543–1548. 10.1002/ptr.2795
Meddah B., Ducroc R., Faouzi M.E., Eto B., Mahraoui L., Benhaddou-Andaloussi A., Martineau L.C., Cherrah Y., Haddad P.S. 2009. Nigella sativa inhibits intestinal glucose absorption and improves glucose tolerance in rats. J Ethnopharmacol. 121(3): 419–424. 10.1016/j.jep.2008.10.040
Meilgaard M.C., Civille G.V., and Carr B.T. 2007. Sensory Evaluation Techniques, 4th edn. CRC Press, Boca Raton, FL. pp. 407–412. 10.1201/b16452
Murlidhar M., and Goswami T.K. 2012. A review on the functional properties, nutritional content, medicinal utilization and potential application of fenugreek. J Food Process Technol. 3(9): 1–10. 10.4172/2157-7110.1000181
Neelakantan N., Narayanan M., de Souza R.J., van Dam R.M. 2014. Effect of fenugreek (Trigonella foenum-graecum L.) intake on glycemia: a meta-analysis of clinical trials. Nutr J. 13(1): 1–11. 10.1186/1475-2891-13-7
Qidwai W., Hamza H.B., Qureshi R., and Gilani A. 2009. Effectiveness, safety, and tolerability of powdered Nigella sativa (kalonji) seed in capsules on serum lipid levels, blood sugar, blood pressure, and body weight in adults: results of a randomized, double-blind controlled trial. J Altern Complem Med. 15(6): 639–644. 10.1089/acm.2008.0367
Rchid H., Chevassus H., Nmila R., Guiral C., Petit P., Chokaïri M., and Sauvaire Y. 2004. Nigella sativa seed extracts enhance glucose-induced insulin release from rat-isolated Langerhans islets. Fundam Clin Pharmacol. 18(5): 525–529. 10.1111/j.1472-8206.2004.00275.x
Robert S.D., Ismail A.A., and Wan Rosli W.I. 2014. Trigonella foenum-graecum seeds lowers postprandial blood glucose in overweight and obese individuals. J Nutr Metab. 2014: 964873. 10.1155/2014/964873
Sobhi W., Stevigny C., Duez P., Calderon B.B., Atmani D., and Benboubetra M. 2016. Effect of lipid extracts of Nigella sativa L. seeds on the liver ATP reduction and alpha-glucosidase inhibition. Pak J Pharm Sci. 29(1): 111–117.
Sun L., Ranawana D.V., Leow M.K., Henry C.J. 2014. Effect of chicken, fat and vegetable on glycaemia and insulinaemia to a white rice-based meal in healthy adults. Eur J Nutr. 53(8): 1719–1726. 10.1007/s00394-014-0678-z
Thomas J.E., Bandara M., Lee E.L., Driedger D., and Acharya S. 2011. Biochemical monitoring in fenugreek to develop functional food and medicinal plant variants. N Biotechnol. 28(2): 110–117. 10.1016/j.nbt.2010.09.001
Wani S.A., and Kumar P. 2018. Fenugreek: a review on its nutraceutical properties and utilization in various food products. J Saudi Soc Agr Sci. 17(2): 97–106. 10.1016/j.jssas.2016.01.007
Zenel A.M., and Stewart M.L. 2015. High amylose white rice reduces post-prandial glycemic response but not appetite in humans. Nutrients. 7(7): 5362–5374. 10.3390/nu7075225
Zhang Z., Kane J., Liu A.Y., and Venn B.J. 2016. Benefits of a rice mix on glycaemic control in Asian people with type 2 diabetes: a randomised trial. Nutr Diet. 73(2): 125–131. 10.1111/1747-0080.12158